
Congenital Aganglionic Megacolon (Hirschsprung Disease)
Introduction
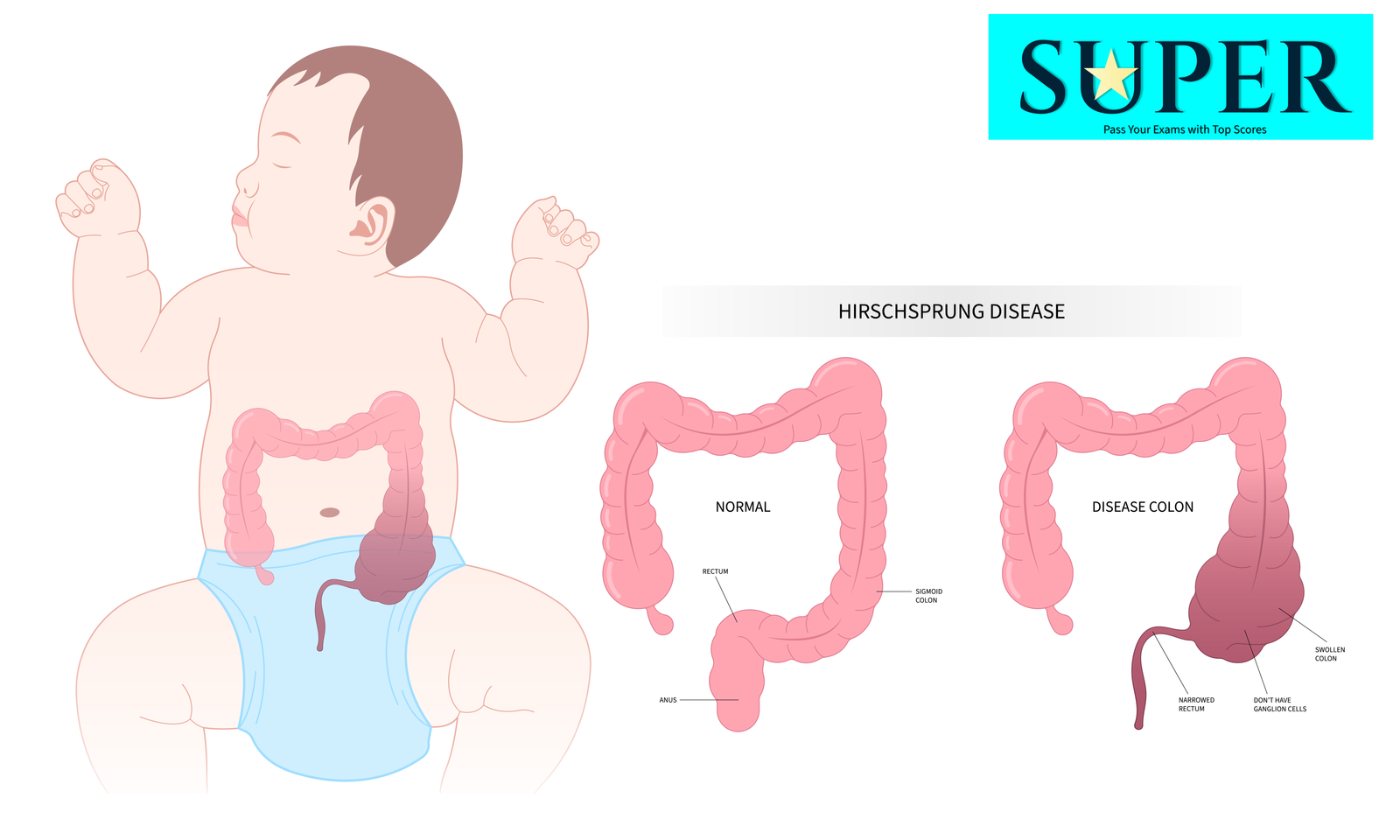
Congenital aganglionic megacolon, or Hirschsprung disease (HD), is a congenital disorder characterized by the absence of ganglion cells in the distal bowel due to neural crest cell migration failure during fetal development. This results in a lack of coordinated peristalsis and functional obstruction.
Pathophysiology
- Neural Crest Cell Migration Failure:
- Ganglion cells in the submucosal (Meissner’s) and myenteric (Auerbach’s) plexuses fail to develop in the affected bowel segment.
- Aganglionic Segment:
- Most commonly involves the rectosigmoid region (80% of cases).
- Can extend proximally in severe cases.
- Functional Obstruction:
- The aganglionic segment remains tonically contracted, causing proximal bowel dilation and distension.
Epidemiology
- Incidence: 1 in 5,000 live births.
- Male-to-female ratio: 4:1.
- Associated with Down syndrome and other genetic syndromes.
 Clinical Features
Clinical Features
- Neonates:
- Failure to pass meconium within the first 24 hours of life (classic sign).
- Abdominal distension.
- Bilious vomiting or feeding intolerance.
- Infants/Children:
- Chronic constipation or infrequent bowel movements.
- Foul-smelling, ribbon-like stools.
- Failure to thrive with poor weight gain and hypoproteinemia.
- Complications:
- Enterocolitis: Life-threatening complication with fever, explosive diarrhea, and sepsis.
- Bowel perforation and peritonitis in severe cases.
Diagnosis
- Clinical Assessment:
- History of delayed meconium passage, chronic constipation, or abdominal distension.
- Digital rectal examination:
- Anal canal and rectum devoid of fecal material despite retained stool on imaging.
- Squirt sign: Gush of flatus and stool as the finger is withdrawn if the aganglionic segment is short.
- Imaging Studies:
- Abdominal X-ray: Shows distended bowel loops with a transition zone.
- Contrast enema: Identifies the transition zone between the dilated normal bowel and the contracted aganglionic segment.
- Definitive Diagnosis:
- Rectal Biopsy:
- Absence of ganglion cells in the submucosal and myenteric plexuses.
- Nerve trunk hypertrophy and increased acetylcholinesterase activity on special staining.
- Rectal Biopsy:
- Anorectal Manometry (Optional):
- Failure of the internal anal sphincter to relax.
Management
- Definitive Treatment:
- Surgical resection of the aganglionic segment (e.g., Swenson, Soave, or Duhamel procedures).
- Pull-through procedure to connect normal innervated bowel to the anus.
- Preoperative Care:
- Manage obstruction with rectal irrigation and bowel decompression.
- Treat enterocolitis if present with IV fluids and antibiotics.
- Postoperative Care:
- Monitor for complications such as:
- Anastomotic strictures.
- Leakage.
- Recurrent enterocolitis.
- Monitor for complications such as:
Prognosis
- Most children achieve good bowel function after surgery.
- Long-term issues may include:
- Constipation.
- Soiling.
- Recurrent enterocolitis in some cases.
SUPERPoint: Hirschsprung disease results from aganglionic segments in the colon, typically presenting with failure to pass meconium, and is definitively treated with surgical resection.
SUPERFormula: Days old baby is brought by parents because he failed to pass meconium, has abdominal distention and bilious vomiting + caused by failure of neural crest cell migration, leading to absent ganglion cells in the distal bowel + most commonly affects the rectosigmoid region + diagnosis confirmed by rectal biopsy showing absent ganglion cells and hypertrophied nerve fibers + managed with surgical resection of the aganglionic segment and pull-through procedures = Congenital Aganglionic Megacolon (Hirschsprung Disease).