
Graft-versus-host disease (GVHD)
Graft-versus-host disease (GVHD)
Graft-versus-host disease (GVHD) is a life-threatening complication that can occur after certain stem cell or bone marrow transplants.
-it is the primary cause of morbidity and mortality after hematopoietic cell transplantation
-30 to 70 percent of transplant recipients develop GVHD
Time course: Acute GVHD usually happens in the first 100 days after an allogeneic stem cell transplant. Chronic GVHD usually starts 100 or more days after the transplantation. However, this classification is artificial and unsatisfactory.
Mechanism: Immunocompetent cytotoxic T cells from the donor proliferate in the immunocompromised host and reject host cells as ‘foreign’ leading to inflammatory damage to the immune system, skin, liver, and GI tract.
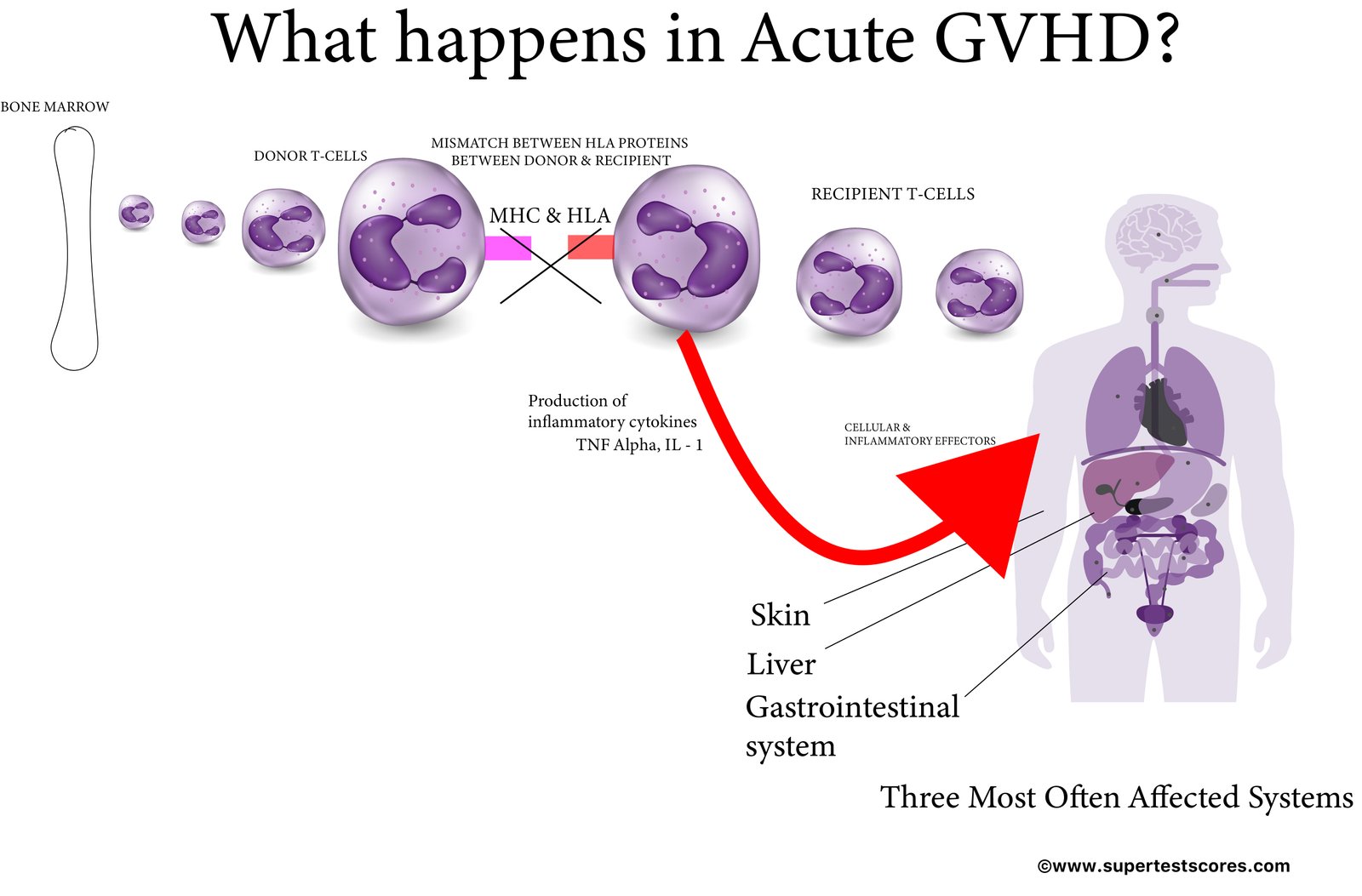
Symptoms & Signs:
Acute Graft-versus-Host Disease
-most often affects the skin, gastrointestinal (GI) tract and liver. So, if you see skin rash, diarrhea and bilirubin elevation after allogeneic transplantation, think of acute GVHD.
Skin: Skin is the most common organ affected in patients with GVHD and most common symptom of GVHD of the skin is maculopapular rash associated with itching, burning and redness of the skin; itching followed by folliculocentric or morbilliform rash often beginning on the trunk and spreading out.
GI tract: the most classic symptom of GVHD of the GI tract is diarrhea; nausea, vomiting and abdominal pain
Liver: cholestatic Jaundice, confusion, ascites
Chronic Graft-versus-Host Disease
-60 – 70% who receive allogeneic transplant develop chronic GVHD
Eyes: Dry eyes, sicca syndrome, photophobia, cicatricial conjunctivitis
Mouth: Dry mouth, mouth sores, dysphagia, mucoceles, Wickham striae of the palate, restrictions of mouth opening from sclerosis
Skin: dry rash, dyspigmentation, new onset alopecia, poikiloderma, lichen-planus-like eruptions or sclerotic features, plaques,extensive erythema, scaling, ichthyosis, ‘pipe stem’ legs, ‘groove sign’, spontaneous loss of pigment in a ‘leopard’ distribution
Nails: hard, brittle nails, nail dystrophy
Hair: loss of hair on the head
GI tract: nausea, vomiting, diarrhea, loss of appetite, esophageal web or strictures
Lungs: wheezing, persistent cough, shortness of breath, pleural effusions
Heart: pericarditis
Liver: Jaundice, abdominal swelling
Muscles and joints: sclerosis, muscle weakness, cramps, limited wrist and finger extension ‘prayer sign’
Genitals: vaginal dryness, irritation, ulceration
Marrow: anemia, thrombocytopenia, neutropenia
Secondary infections: cytomegalovirus (CMV) pneumonia, varicella-zoster
Diagnosis: CBC, liver function tests, CXR, biopsy etc
Biopsy: presence of necrotic keratinocytes accompanied by a dermal lymphocytic infiltrate (usually sparse) and basal vacuolar interface alteration
Treatment:
The gold standard for treatment of GVHD: topical or systemic steroids
Other treatments: Plasmapheresis, extracorporeal photopheresis (ECP), Cyclosporine, methotrexate, cyclophosphamide,mycophenolate, sirolimus, biologics
Prevention: the primary pharmacologic strategy to prevent GVHD is the inhibition of the cytoplasmic enzyme, calcineurin, which is critical for the activation of T cells. The calcineurin inhibitors include cyclosporine and tacrolimus.
References:
https://www.lls.org/treatment/types-treatment/stem-cell-transplantation/graft-versus-host-disease